Philosophy has a very small role in medical practice.I would be writing in my speaking tree (spiritual site) blog if I had to share the soul search in my midlife!
In this blog, I want to describe my role as an ENT doctor & what I specialise in.
ENT is a diverse speciality that continues to grow & expand.
ENT is considered a surgical speciality.However let me bring to your notice that an ENT Surgeon does a lot of general medical practice as well.Its not all surgery.
Statistics say around 30% of general medical visits & about 40% of pediatrician visits are with ENT issues like sore throats,allergies,sinusitis etc.
ENT's play a role in multi disciplinary teams like assessments of headaches,vertigo,tinnitus,rheumatological disorders,snoring & sleep apnoea, special needs children.....the list is exhaustive.
During the post graduate training we systematically acquire the knowledge of all & an ENT can assess & diagnose all of below.When it comes to clinical practice,we specialise in our areas of interest or what we are best at!
Following are the areas an ENT can specialise.
1.Otology which includes ear diseases,deafness & Neuro otology & Audiology
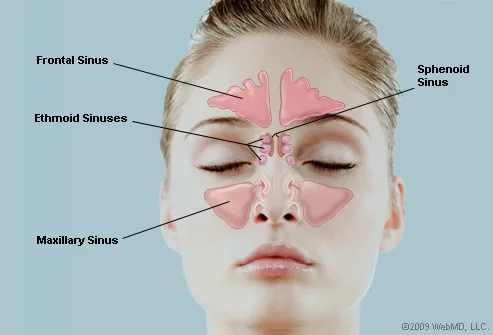
2.Rhinology which includes paranasal sinuses & advanced nasal endoscopic work like pituitary & orbit
3.Laryngology which includes phonosurgery,airway & swallowing disorders
4.Pediatric Otolaryngology
5.Head & Neck surgery includes benign & malignant tumors
6.Facial plastic & reconstructive surgery
Still more interested groups work on Preventive ENT & Geriatric ENT.
My special interests are
I have been successfully running opd based diagnostics for children with airway problems.Our swallowing assessments in opd (FEEST) are not only popular with neurologists but also with patients & their families.
The surgical work where I would like to concentrate will be ear surgeries & deafness.The endoscopic work which i do includes sinus surgeries & with neurosurgeons approach to pituitary & orbit.
The ever evolving medical practice needs updating & constant learning !The learning never stops.
Here as soon as you achieve a goal... new technique comes & a new goal is automatically set up for you.This is different from philosophy ....I can never say I have achieved all & have to keep updating.
The sky's the limit.......or may be even further,as I read somewhere ....
Merry Christmas & a very Happy New Year 2013...think ahead!
 |
| Sharing my expereinces at a working women's meet organised in Bangalore ! |
ENT is a diverse speciality that continues to grow & expand.
ENT is considered a surgical speciality.However let me bring to your notice that an ENT Surgeon does a lot of general medical practice as well.Its not all surgery.
Statistics say around 30% of general medical visits & about 40% of pediatrician visits are with ENT issues like sore throats,allergies,sinusitis etc.
ENT's play a role in multi disciplinary teams like assessments of headaches,vertigo,tinnitus,rheumatological disorders,snoring & sleep apnoea, special needs children.....the list is exhaustive.
During the post graduate training we systematically acquire the knowledge of all & an ENT can assess & diagnose all of below.When it comes to clinical practice,we specialise in our areas of interest or what we are best at!
Following are the areas an ENT can specialise.
1.Otology which includes ear diseases,deafness & Neuro otology & Audiology
2.Rhinology which includes paranasal sinuses & advanced nasal endoscopic work like pituitary & orbit
3.Laryngology which includes phonosurgery,airway & swallowing disorders
4.Pediatric Otolaryngology
5.Head & Neck surgery includes benign & malignant tumors
6.Facial plastic & reconstructive surgery
Still more interested groups work on Preventive ENT & Geriatric ENT.
My special interests are
- Otology including surgeries for deafness & Cochlear Implants
- Endoscopic Sinus Surgery
- Pediatric ENT
- Swallowing & Speech disorders
I have been successfully running opd based diagnostics for children with airway problems.Our swallowing assessments in opd (FEEST) are not only popular with neurologists but also with patients & their families.
The surgical work where I would like to concentrate will be ear surgeries & deafness.The endoscopic work which i do includes sinus surgeries & with neurosurgeons approach to pituitary & orbit.
The ever evolving medical practice needs updating & constant learning !The learning never stops.
Here as soon as you achieve a goal... new technique comes & a new goal is automatically set up for you.This is different from philosophy ....I can never say I have achieved all & have to keep updating.
The sky's the limit.......or may be even further,as I read somewhere ....
Merry Christmas & a very Happy New Year 2013...think ahead!